



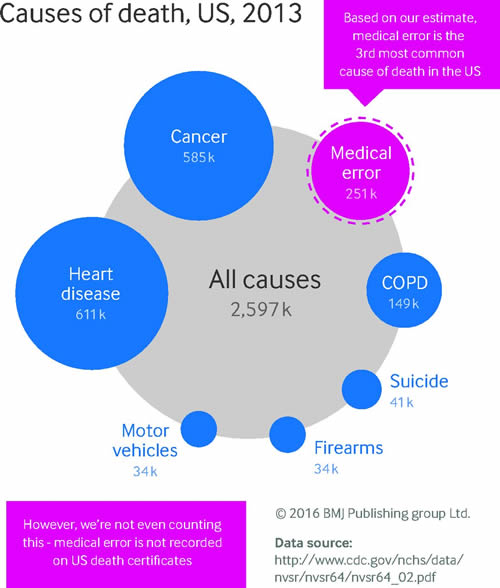
Social media and mainstream media is abuzz with this article in BMJ by Martin A Makary and Michael Daniel entitled “Medical error—the third leading cause of death in the US.” This image summarizes the headlines most people wrote:
While this makes for a great headline, most of the journalists and those in the media evaluating the BMJ article do like they usually do and run the headline without actually digging into the details of the study itself. Lucky for us, David Gorski, has published a really great analysis of the article on the Science-Based Medicine blog. I won’t summarize it here, since you should go and read David’s article in full. We’ll be here when you get back.
What everyone acknowledges is that medical errors take the lives of many in the US Health System. In fact, it happens in every health system. What’s also clear from this discussion is that there are A LOT of complexities associated with how you define when a death was caused by medical error, what is defined as a medical error, etc etc etc. David’s article above finishes with this summary on the importance of patient safety and decreasing death due to medical errors which is the point I think we should take from it all:
Over the last three years, I’ve learned for myself from firsthand experience just how difficult it is to improve the quality of patient care. I’ve also learned from firsthand experience that nowhere near all adverse outcomes are due to negligence or error on the part of physicians and nurses. None of this is to say that every effort shouldn’t be made to improve patient safety. Absolutely that should be a top health care policy priority. It’s an effort that will require the rigorous application of science-based medicine on top of expenditures to make changes in the health care system, as well as agreement on exactly how to define and measure medical errors. After all, one death due to medical error is too much, and even if the number is “only” 20,000 that is still too high and needs urgent attention to be brought down. Unfortunately, I also know that, human systems being what they are, the rate will never be reduced to zero. That shouldn’t stop us from trying to make that number as close to zero as we can.
Unfortunately, I believe that false headlines with inflated numbers don’t help us understand the real problem and address it. The inflated numbers from the so called “study” just cause us to confuse the issues. The numbers really don’t pass the “smell test” on a number of levels. Not the least of which, from my perspective, is that we don’t have more medical malpractice lawsuits. In this sue happy society, if there were 251k deaths due to medical error, we’d have many more medical malpractice lawsuits out there. David explains a bunch more reasons why the numbers don’t make sense and why they’re really hard to calculate, so go and read those if you want a more detailed analysis.
Gong back to the earlier quote. Even if the number was 20,000, that’s still far too many. We know medical errors cause death and we should work hard to prevent that from happening. Since I write from a tech perspective, I’m interested in thinking about how technology could impact these medical error rates.
From a tech perspective, I always find it interesting to read stories about the way EHR software can help prevent medical errors. The basic analysis usually points to things like drug to drug interaction checking, drug to allergy interaction checking, and other clinical decision support tools. No doubt simple checks like this can have an impact on the number of medical errors in a healthcare organization. We’ll leave the discussions of alert fatigue for another discussion.
Very few people would argue against the concept that having the right information at the right time will help doctors and nurses reduce medical errors. Ideally, that’s what technology should help facilitate. Plus, technology should help analyze massive amounts of health data (both personal and general) in order to facilitate the provider in their care of the patient. In many cases, that’s exactly what technology can and does do for healthcare. However, we’re not living in an ideal world. Technology can also increase the number of medical errors when implemented poorly or improperly.
In some cases, EHR software perpetuates misinformation and leads to providers having the wrong information at the wrong time. Sometimes the clinical decision support algorithms fail. I could go on and on about the potential issues. These are a problem and now that EHR software is a major part of most health systems, we’re going to see the number of medical errors due to EHR software increase. However, in doing so, we shouldn’t forget that paper had its own medical error issues as well.
Another major cause of medical errors related to EHR software is when providers create an over reliance on the software for clinical decision making. This concern is often couched as “new doctors don’t know how to see patients without an EHR.” I think this concern only partially explains the risk of medical errors that we could experience if we’re not careful with our over reliance on technology in the care we provide patients.
Just this weekend I had this experience in my own personal life. We were headed to a new restaurant on Saturday night. We plugged the address into the GPS and started following the instructions it gave us to get to the restaurant. After turning into an apartment complex, we knew that we’d relied a little too much on technology and it had led us astray.
The banter between my wife and I was telling. As the GPS told us to turn into the apartment complex I told my wife that something didn’t feel right about these directions. My wife told me that it said to turn there. It was easy for me to succumb to my wife’s reliance on technology and not follow my own intuition and experience to navigate us a better direction.
In my wife and I’s case, nothing too serious was on the line (although the kids were getting antsy in the back of the car). Sure, it took us about 5 more minutes to get to the restaurant, but we made it without any major harm. The same isn’t true in healthcare where if providers aren’t careful, their over reliance on technology can cause medical errors that could even lead to loss of life. Plus, group think about technologies ability (or inabilities) can also cause trouble.
Like most things in life, we can take any of these approaches too far. We can’t be irrational about any specific approach since these are complex problems which require a detailed approach to understanding and mitigating their impact. Sometimes technology can be the solution to medical errors, but it can also be the problem if we’re not careful. It always takes the right balance to make sure we’re reducing medical errors as much as possible while not causing new ones.








It seems to me that all the conversation spent parsing this (and previous) analyses not only miss the point, but by distracting attention and energy from the real issue(s):
1. We unambiguously signal that errors and resulting harm are rare and inconsequential by having no functional system to collect, analyze and use data.
2. We are making few efforts and less progress shifting to a culture that sees quality and safety as a team product and uses both errors and near misses to improve team performance.
3. The default is still to assume that errors are a result of an individual doing the wrong thing within a system that is properly designed, when the truth is much closer to a system making it hard to do the right thing.
Instead of yammering away about this report, we should be working on the real problem.
Peter Elias, MD
While establishing direct causality between medical errors and mortality is non trivial and I agree with that. I have to respectfully disagree with your smell test of there being not enough malpractice law suits. A lot of the errors were not preventable and malpractice suits according to data are typically filed when the caregivers are kept in the dark about what is going on and what decisions are being taken.
Great advice Peter. Thanks for adding to the conversation.
Until medical information originates from each of us continuously, there will be unpleasant surprises to medical professionals. The way we feel, the meds, supplements, food and recreational substances we ingest are critical to the efficiency of our evolving world of medical science. This can be done. We will get there.
“Medical errors” have impacted my life both personally and professionally. I lost my father too soon due to a glaring act of omission. As a patient myself, a broken cannula was left in my knee post-ACL reconstruction. I did not file lawsuits in ether instance for several reasons;
Both my father’s cardiologist and my ortho were wonderful doctors and kind, compassionate human beings. My father absolutely revered his doctor without whom, his quality of life would have suffered.Dad was more interested in quality than quantity. The error was a failure of nursing to administer a vital med. In my case, my surgeon/friend listened to me when I insisted that an object had been left in my knee. He re-opened my knee and retrieved the fragment. He then apologized and stated; “Thank God you are a physical therapist and not a lawyer”. I chided, “Yes, but I know many lawyers!”.
Some closing thoughts; not all errors that are labeled “medical” are medical. In fact, many if not most are “Administrative”. Of course, they flow from medical care. My point is, lawsuits are not the answer even though for some “blood money” is healing. In both cases, I notified hospital QA/CQI personnel not attorneys.
Some readers may no doubt and understandably believe that my bias as a medical professional is why I did not go to court. I did not sue because both doctors did their best given the circumstances, both were good listeners and well intended healers. We can’t heal them all, but we can do our very best in this art we call medicine.