



It’s an unfortunate truth that the health care system is not fool proof, and mistakes happen. Many of these mistakes happen because of paperwork that is lost, unreadable, or misplaced. Even with the implementation of EMRs across the country, many healthcare providers are still relying on paper for many aspects of their practice. Referral MD created an infographic that shows some of the current problems in healthcare related to using paper documents:
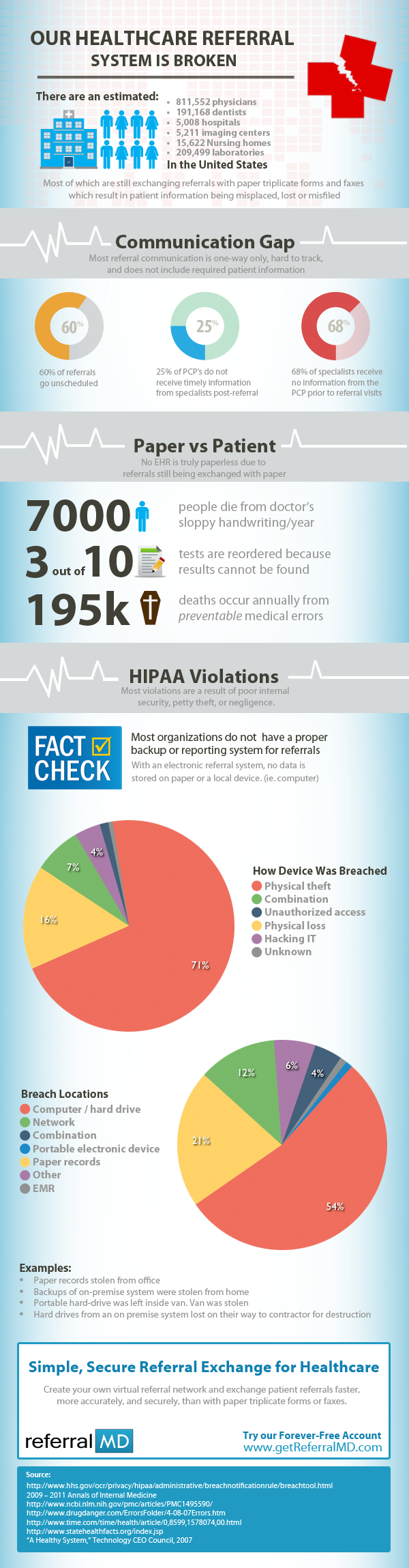
Pretty scary, if you ask me. Doctor’s are notorious for having terrible handwriting, but 7000 patients die a year because of it? And 30 percent of tests have to be reordered because the orders were misplaced? These statistics are startling, in large part because they are preventable. Those are only two of the facts presented in this infographic, and in combination with everything else, it makes me wonder why anyone that has an EMR would still use paper, and why the practices that don’t use EMRs haven’t started. It makes me not want to trust the system even more.
I can see how patients and doctors alike may find it hard to switch over. When I wasn’t given a physical, paper prescription to take to the pharmacy to get my son’s medication, I was a bit taken back, but it made things so much easier when I actually arrived at the pharmacy. I compare that to the many prescriptions and lab orders I lost during my pregnancy because I set it down and forgot to pick it up again, never to find it again until months later while doing some cleaning. It made me really wish my OB/GYN had electronic documents more incorporated into his practice. I’m curious to see if he has any EMR at all. Since he’s been a doctor for 40+ years, maybe he’s having a hard time making the switch.
It’s one thing if a person dies from a terminal illness, but to pass away because of a preventable mistake is uncalled for. I realize that no one is perfect. Everyone makes mistakes. But when a mistake could mean someone dying, a patient’s information being misused, or a HIPAA violation occurring, something is wrong. Hopefully as EMRs become better and more practices have them, paper documentation will become a thing of the past, and these mistakes, breeches, and all other issues that are related to using paper, will go that way as well.







